Surgery is reserved for patients who need arm strength, are concerned with cosmetics of the balled up biceps, or who have pain that won't go away.
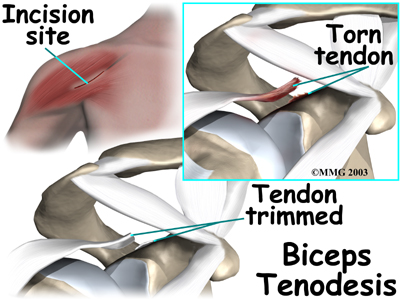
Biceps Tenodesis
Biceps tenodesis is a surgery to anchor the ruptured end of the biceps tendon. A common method, called the keyhole technique, involves anchoring the ruptured end to the upper end of the humerus. The keyhole describes the shape of a small hole made by the surgeon in the humerus. The end of the tendon is slid into the top of the keyhole and pulled down to anchor it in place.
The surgeon begins by making an incision on the front of the shoulder, just above the axilla (armpit). The overlying muscles are separated so the surgeon can locate the damaged end of the biceps tendon. The end of the biceps tendon is prepared by cutting away frayed and degenerated tissue.
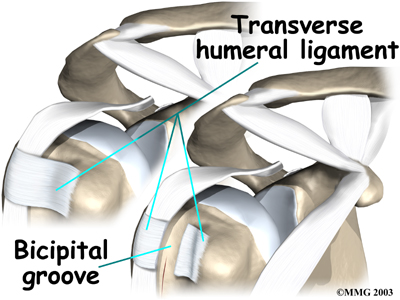
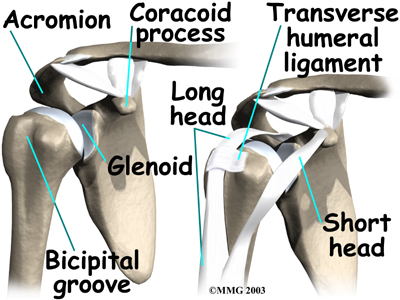
The transverse humeral ligament is split, exposing the . An incision is made along the floor of the bicipital groove. The bleeding from the incision gets scar tissue to form that will help anchor the repaired tendon in place.
A burr is used to form a cavity within the bicipital groove. The top of the cavity is round. The bottom is the slot of the keyhole. It is made the same width as the biceps tendon.
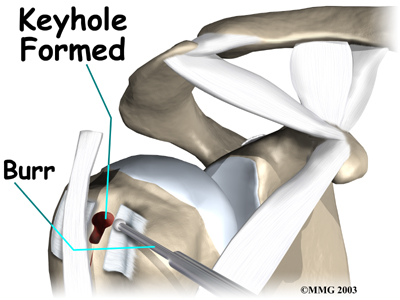
The surgeon rolls the top end of the biceps tendon into a ball. Sutures are used to form and hold the ball. The elbow is bent, taking tension off the biceps muscle and tendon. The surgeon pushes the tendon ball into the top part of the keyhole. As the elbow is gradually straightened, the ball is pulled firmly into the narrow slot in the lower end of the .

The surgeon tests the stability of the attachment by bending and straightening the elbow. When the surgeon is satisfied with the repair, the skin incisions are closed, and the shoulder is placed in a protective sling.
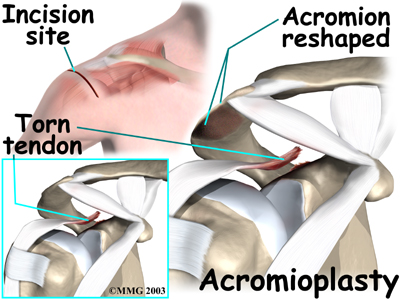 Acromioplasty and Direct Tenodesis
Acromioplasty and Direct Tenodesis
This procedure may be used for younger patients who've had a recent traumatic biceps rupture, have problems with impingement, and who have an injured rotator cuff.
involves cutting and reshaping the acromion, the bone that forms the top part of the shoulder. Some surgeons will also sever the corocohumeral ligament, which arches over the top of the shoulder joint. These steps relieve pressure on the tissues between the ball of the humerus and the acromion, including the biceps and rotator cuff tendons. For this reason, this procedure is sometimes called subacromial decompression. The ruptured end of the biceps is then anchored to the upper end of the humerus. This is called direct tenodesis.
The surgeon begins by making an incision across the top of the shoulder. The shoulder muscles are separated to expose the top of the humerus. Bone spurs are removed, along with part of the acromion. The surgeon then smooths the rough ends of the bone.
After the acromioplasty procedure, the surgeon focuses on the biceps tendon. When the bicipital groove is in view, the transverse humeral ligament is cut. Next, an osteotome is used to open the joint capsule and create a trough next to the bicipital groove. Three small holes are drilled along each side of the trough. The surgeon places the loose end of the biceps tendon in the new groove.

Sutures are woven into one drill hole, through the tendon, and out the opposite drill hole. This is repeated for the remaining two sets of drill holes. Next, the top end of the ruptured tendon is cut off. Finally, the are firmly secured.
When the surgeon is satisfied with the repair, the transverse humeral ligament and joint capsule are sutured, followed by the skin incision. The arm is bent at the elbow and placed in a light splint that is to be worn for four weeks after surgery.
Portions of this document copyright MMG, LLC.


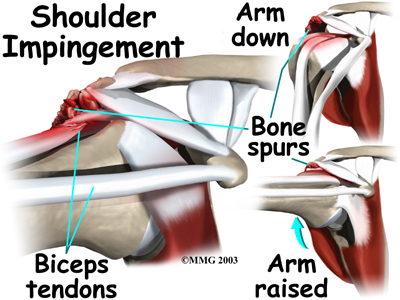 Biceps ruptures generally occur in people who are between 40 and 60 years old. People in this age group who've had shoulder problems for a long time are at most risk. Often the biceps ruptures after a long history of shoulder pain from tendonitis (inflammation of hte tendon) or problems with
Biceps ruptures generally occur in people who are between 40 and 60 years old. People in this age group who've had shoulder problems for a long time are at most risk. Often the biceps ruptures after a long history of shoulder pain from tendonitis (inflammation of hte tendon) or problems with 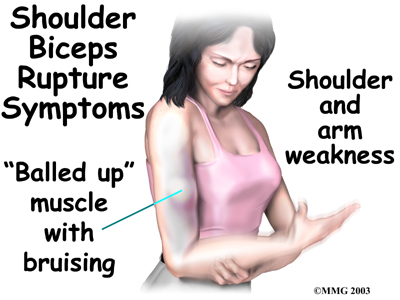
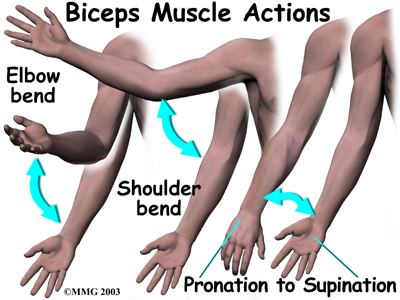
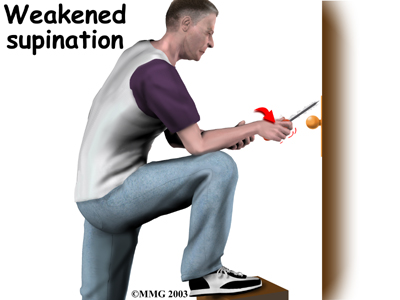 Not having surgery usually only results in a moderate loss of strength. The short head of the biceps is still attached and continues to supply strength to raise the arm up. Flexion of the elbow may be affected, but supination (the motion of twisting the forearm such as when you use a screwdriver) is usually affected more. Not repairing a ruptured biceps reduces
Not having surgery usually only results in a moderate loss of strength. The short head of the biceps is still attached and continues to supply strength to raise the arm up. Flexion of the elbow may be affected, but supination (the motion of twisting the forearm such as when you use a screwdriver) is usually affected more. Not repairing a ruptured biceps reduces