Non-surgical Rehabilitation
Spinal myelopathy is a serious condition. If your condition is causing significant problems or is rapidly getting worse, we may not begin with nonsurgical treatments and instead recommend you see a doctor to explore surgical options immediately. If the symptoms are mild, your Emerald Hills Physio & Sports Clinic physiotherapist may initially try nonsurgical treatment to see if the symptoms improve.
Although the length of treatment is different for each individual, as a general guideline, Emerald Hills Physio & Sports Clinic patients with mild symptoms of cervical myelopathy typically undergo rehabilitation for three to six months.
At first, we may suggest immobilizing the neck. Keeping your neck still for a short time can calm inflammation and pain. We instruct patients to restrict their daily activities by avoiding heavy and repeated motions of the neck, arms, and upper body.
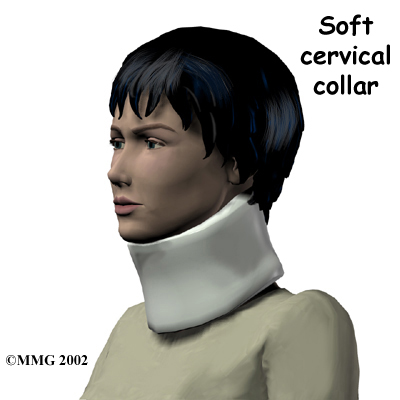
Our therapist may also prescribe a . The collar is a padded ring that wraps around the neck and is held in place by a Velcro strap. Patients wear the collar during waking hours, usually for up to three months. Then they slowly begin to taper the amount of time they wear it each day. After wearing a neck brace for up to three months, most patients slowly resume their routine activities.
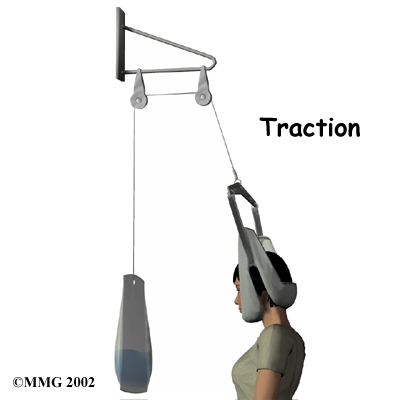
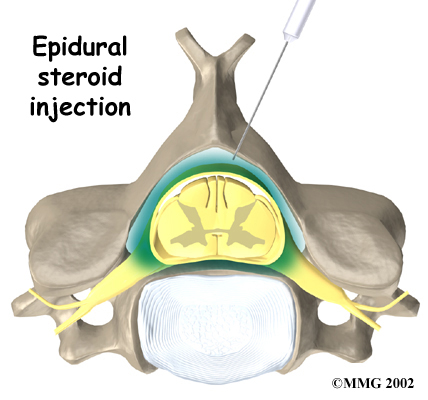
After initial immobilization, our first treatments are used to ease pain and inflammation. Our physiotherapist may use electrical stimulation treatments to help calm your muscle spasms and pain. We might recommend traction as a way to gently stretch your joints and the muscles of your neck. This can be done using a machine with a or our physiotherapist can apply the traction pull by hand.
Post-surgical Rehabilitation
Some patients leave the hospital shortly after surgery. Other surgeries require patients to stay in the hospital for a few days. Physiotherapist routinely see patients for treatment in their hospital room after surgery. Therapy sessions are designed to help patients learn to move and to begin doing routine activities without putting extra strain on the neck.
During recovery from surgery, you may have to be placed in a halo vest or rigid neck brace. These braces are used to restrict motion in the neck to allow the fusion to heal. Patients generally need to be extremely cautious about overdoing activities in the first few weeks and months after surgery.
Most patients spend some time rehabilitating at home. Bone fusion may take several months. When the health care providers are absolutely certain that the bones have fused together, patients are able to discontinue using the neck brace or halo vest.
After being in a rigid neck brace for four to six months, patients are often weak and deconditioned. At Emerald Hills Physio & Sports Clinic, our physiotherapists can work with you on neck movement, strength, and general conditioning.
As our physiotherapy sessions come to an end, we may help you with decisions about getting back to work. Ideally, patients are able to go back to their previous activities. However, some patients may need to modify their activities to avoid future problems.
At Emerald Hills Physio & Sports Clinic, our goal is to help you keep your pain under control, improve your range of motion, and maximize strength and control in your neck. When your recovery is well under way, regular visits to our office will end. We will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.
Emerald Hills Physio & Sports Clinic provides services for physiotherapy in Sherwood Park.
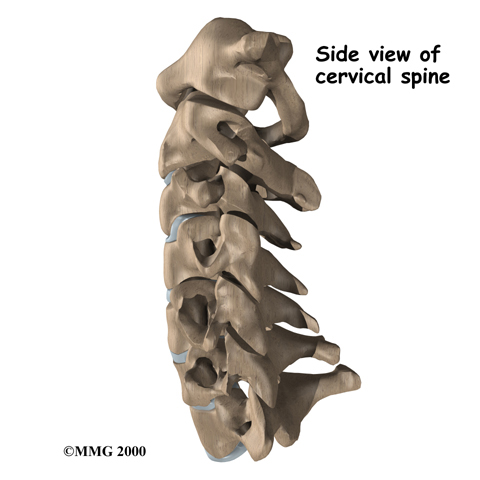 The spine is made of a column of bones. Each bone, or vertebra, is formed by a round block of bone, called a vertebral body. A bony ring attaches to the back of the vertebral body, forming a canal.
The spine is made of a column of bones. Each bone, or vertebra, is formed by a round block of bone, called a vertebral body. A bony ring attaches to the back of the vertebral body, forming a canal.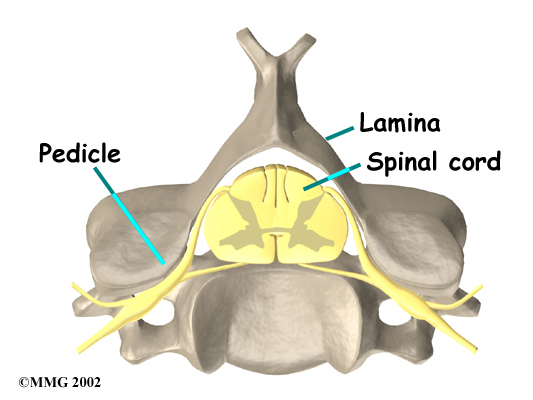 This
This 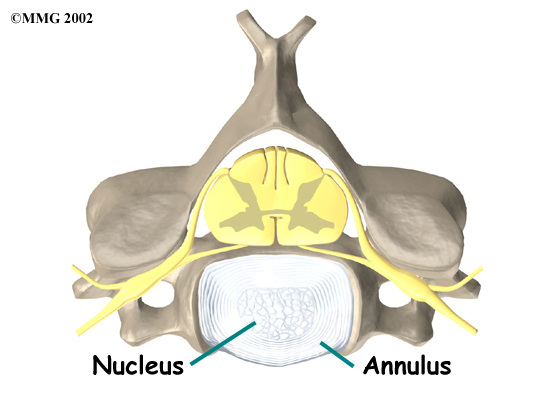
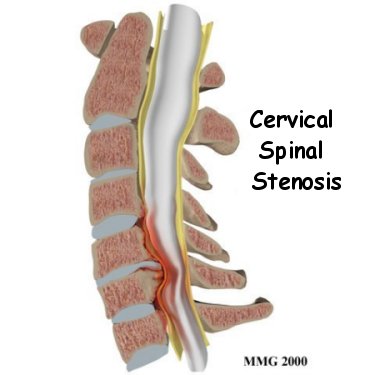
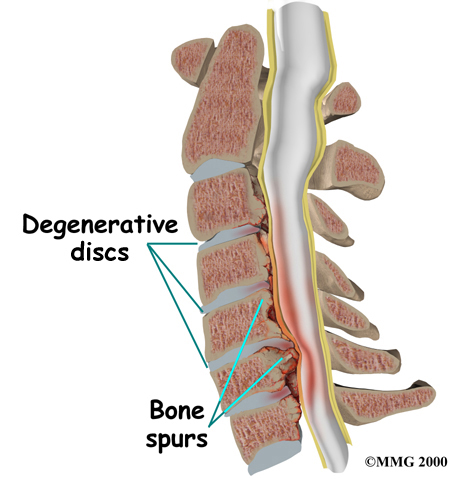 Degeneration is the most common cause of spinal stenosis. Wear and tear on the spine from aging and from repeated stress and strain can cause many problems in the cervical spine. The intervertebral disc can begin to collapse, shrinking the space between vertebrae. Bone spurs may form that protrude into the spinal canal and reduce the space available to the spinal cord. The ligaments that hold the vertebrae together may become thicker and can also push into the spinal canal. All of these conditions
Degeneration is the most common cause of spinal stenosis. Wear and tear on the spine from aging and from repeated stress and strain can cause many problems in the cervical spine. The intervertebral disc can begin to collapse, shrinking the space between vertebrae. Bone spurs may form that protrude into the spinal canal and reduce the space available to the spinal cord. The ligaments that hold the vertebrae together may become thicker and can also push into the spinal canal. All of these conditions 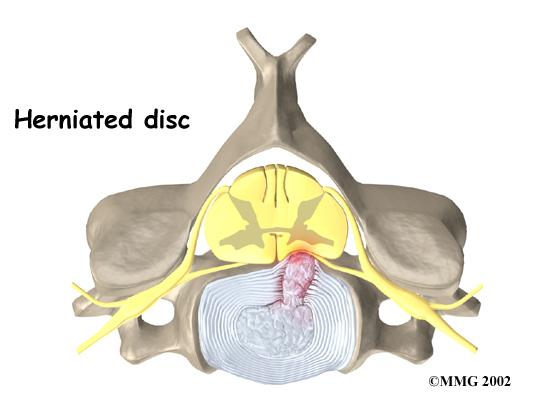
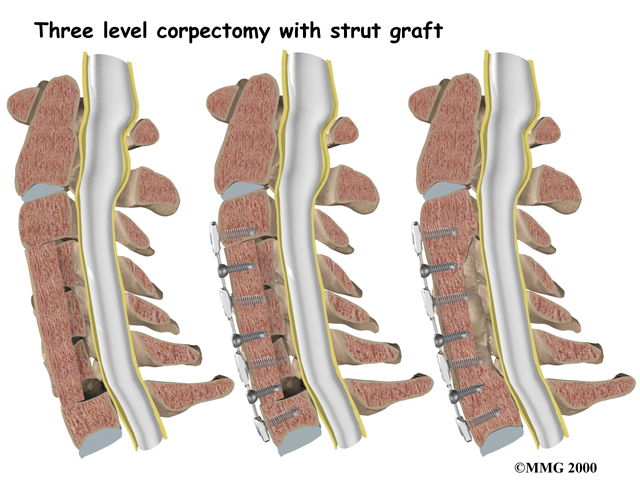
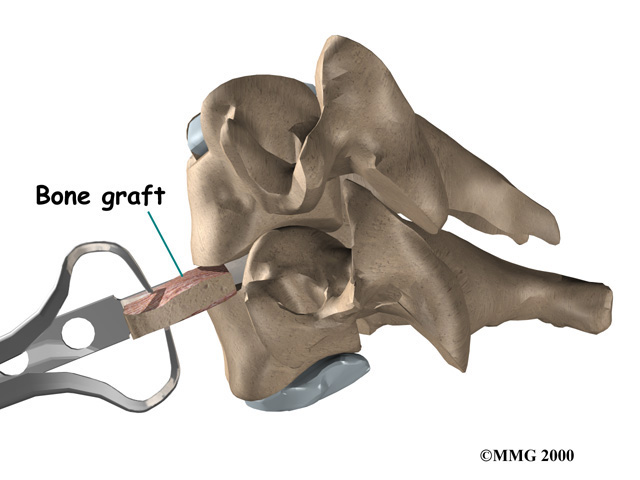 Anterior Cervical Discectomy and Fusion
Anterior Cervical Discectomy and Fusion